|
|
|
Neuromyotonia (NMT) is an uncommon syndrome of spontaneously occurring muscle activity of peripheral nerve origin, which can be triggered by voluntary or induced muscle contraction in which hyperexcitability of peripheral nerves leads to incapacitating muscle twitching, cramps, and weakness. Although NMT may sometimes accompany hereditary neuropathies, most cases are acquired (Isaacs syndrome) and most often as a paraneoplastic syndrome in patients with cancer of the immune system. Antibodies against voltage-gated potassium channels have been detected in some patients. We report two patients with NMT no associated to malignancies that developed acute renal failure while were under treatment with herbal medications by their traditional healer in the former Transkei (South Africa). One of those patients died due to acute renal complications and the other one got a complete recovery of her renal function and further relief of the NMT's manifestation with 1200 mg daily of Gabapentin orally. We have hypothetisized about potassium channelopathy-herbal medication-acute renal failure and after reviewed the medical literature,a similar report is not found. Introduction
Neuromyotonia (NMT) is a rare disorder of unknown cause described by Issacs1 in which hyper excitability of peripheral motor nerves resulting in continuous muscle fiber activity which leads to incapacitating muscle twitching, cramps, and weakness. This syndrome of spontaneously occurring muscle activity can be triggered by voluntary or induced muscle contraction. Although NMT (also known as Isaacs syndrome) may sometimes accompany hereditary neuropathies, most cases are acquired. NMT has been long recognized by several physicians 1 2 3 however its rarity and the variability of its clinical manifestation and ways of presentation is probable the most important reason why its frequently misdiagnosis or confirmation of the diagnosis is delayed. We reported two patients in which after several attends for providing relief throughout the public health sector in the former Transkei (South Africa) they were treated by their traditional healer looking for a better improvement of their neuromuscular disturbances and unfortunately their developed acute renal failure (ARF) probable due to wrong combination of the herbal medications.
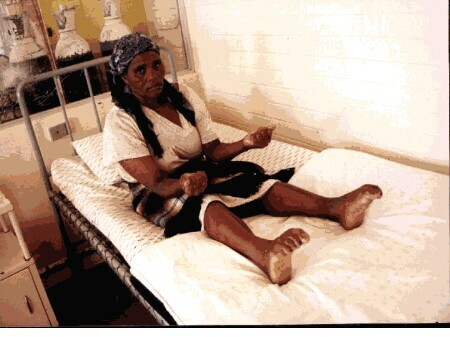
XhM a 49 year old lady came to special medical clinic complaining of dry cough, painful inability to open her hands and to extends her toes which were in flexed position 24 hours a day for the past ten months and scanty urine for five days duration (figure 1). Eight months prior to this admission different medical practitioner in the public and private health sector examined her and a wide range of medications was unsuccessfully prescribed. Following advices from her relatives she went to visit a local traditional healer and a combination herbal medicines such as kankerbos (Sutherlandia frufesces) and Ysterhouttoppe (Dodonaea angustifolia) were prescribed. Complete alleviation of the respiratory manifestation and partial relief of pain on her hands after a few days of treatment is reported.
Two month later, a second visit to the traditional healer was done and a similar combination of herbal medicines was obtained on prescription from another herb seller in town. Apart from cramps and muscle stiffness on the distal region of the limbs, she remained complete a symptomatic until she develops a progressive reduced micturation since 5 days before admission.
On examination weakness on the distal regions in the four limbs, bilateral and symmetrical pseudomyotonia in the hands and feet and increased sweating all over the body even during sleeping time were also observed. Oliguria (less than 300 ml/day) is confirmed and examination of other system revealed unremarkably findings. Laboratory tests showed: Urea (29.3 mmol/L) and creatinine (654 umol/L) and other blood tests were normal. After forced alkaline diuresis and a course of 1200 mg of Gabapentin daily this patient showed a normal renal function and no muscular over activity was detected.
ThB a 21 year old, HIV seropositive male presented to neurology outpatient service with a five years history of generalized weakness, numbness, and tingling sensation of the limbs and also an imperative desire to move his extremities (looking for relief), mainly at night; nine months prior admission he began to complain of muscle twitching on four limbs and inability to get muscle relaxation after any voluntary contraction of the skeletal muscle in hands and feet which becoming worse after a new voluntary muscle contraction. Sleep was disturbed by cramps in his hands when he was 19 years old. One week after the initiation of management with unknown herbal medication at age 20, all clinical manifestation improved but he became progressively worse three months later when his herbal medicines became unavailable from the sellers and from the bush. A week before admission he was trying with another unknown herbal medicines and then he began to complain of scanty urine and worsening of the previous reported clinical features.
General physical examination revealed unremarkably findings and neurological examination showed myokymia and pseudomyotonia on the four limbs, (delay in muscle relaxation was noted after strong hand grips but there was no percussion myotonia)(figure 2). Sensory system examination was normal; muscle tone and deep tendon reflexes were decreased, and muscle power was 4/5 all over the body. Laboratory tests showed: creatinine 2467.9 umol/L, urea: 41.2 mmol/L other blood tests including serum electrolytes, thyroid function test, liver function test, creatine kinase, and full blood count were normal. On the tenth day of admission the patient was found death. The postmortem examination revealed a large pulmonary embolism and an acute tubular interstitial nephritis.
Probable more than 75% of South African use traditional medicines on regular basis, those herbal medicines can be gathered in wild regions or can be bought from herbal sellers in urban areas of South Africa (figure 3) and also previously elaborated product from those herbal can be obtained in "traditional pharmacies" from rural areas (figure 4), those herbal remedies and its constituents play an important role in the management of most of the actual health problems in South Africa in spite of our lack of knowledge about the quantity of medicinally active principles, potential effects, toxicity, and side effect of the various herbs, including genetical variations, mode of collection, drying, storage and final preparation, we also do not know when and how some "similar" herbs are replaying those unavailable ones. Herbal medicines have been reported to be responsible for 0-35% of the cases of ARF in some African countries4 5 6 7 and herbs such as Euphorbia matabelensis and Crotalaria laburnifolia has been associated with ARF8.
Antibody-mediated autoimmune mechanism, possibly directed to peripheral nerve K+ channels, play an important role in etiology of acquired neuromyotonia and we are hypothesized its may be involved in a renal impairment aggravated by toxic mechanisms because similar products does not cause renal damage in other peoples. Neuromyotonia also occurs at increased frequency with certain tumors that are well recognized to produce autoantibody-mediated, paraneoplastic disorders of the peripheral nervous system3. Ten of the 50 or so patients with nuromyotonia reported over the past 2 decades have had a thymoma; 7 patients had myasthenia gravis, others associations including peripheral neuropathy and Hodgkin's lymphoma have been reported9. It is the first report of neuromyotonia and acute renal failure due to herbal intoxication to the medical literature.
The pathogenesis of ARF following herbal medication could be multiple however direct nephrotoxicity has been reported67 the second reported patient was HIV seropositive (CD4 > 350 cells), but how it's influenced on the pathogenesis of acute renal failure is uncertain. NMT usually respond very well to anticonvulsants such as Phenytoin or Carbamazepine, a good response to Gabapentin in one of our patients is also reported. Immunoadsorption plasmapheresis and immunosuppressive drugs are optional treatment of Isaacs' syndrome.10
To confirm the identities and pharmacological characters of the most common used herbal remedies in South Africa is an important priority, adequate regulations and a better control about improper preparations, and combinations is recommended.
1. Isaacs H. A syndrome of continuous muscle-fibre activity. J Neurol Neurosurg Psychiatriy 1961; 24: 319-25
2. Newson-Davis J, Mills KR. Immunological associations of acquired neuromytonia (Isaacs' syndrome). Report of five cases and literature review. Brain 1993 APR; 116(Pt 2): 453-69
3. Ian KH. Acquired Neuromyotonia: A new Autoantibody-Mediated Neuronal Potassium Channelopathy. Amer J Med Sci 2000 APR; 319:209-216
4. Godd, CH. Acute renal failure from Herbal and patent remedies in Black. Clin Nephrol. 1980; 14:128-135
5. Lowenthal, MN, Jones IG, Mohelsky V. Acute renal failure in Zambian women using traditional herbal remedies. J Trop .Med Hyg 1974; 77:190-194
6. Dukes DC et al. Acute renal failure in Central Africa: The toxic effect of traditional African remedies. Cent Afr J Med 1969; 15:71-74
7. Seedat YK: Acute renal failure among Blacks and Indians in South Africa. S. Afr. Med J 1978; 54:427-431
8. Otieno LS, McLigeyo SO, Luta M. Acute renal failure following the use of herbal remedies. East Afr Med J. 1991;13:993-98
9. LahrmannH, et al Acquired neuromyotonia and peripheral neuropathy in a patient with Hodgkin's disease. Muscle Nerve 2001 Jun;24(6):834-8
10. Nakatsuji Y, Kaido M, Sugai F, Nakamori M et al Isaacs' syndrome successfully treated by immunoadsorption plasmapheresis Acta Neurol Scan 200; 102:271-273 |