|
Paneles de Discussión
Paneais de Discussio Comunicaciones libres
Comunicaçoes livres |
Aristolochic acid (formerly Chinese herbs) nephropathyCosyns Jean-Pierre, MD PhDDepartment of Pathology, Medical School, Cliniques Universitaires St-Luc, Université Catholique de Louvain, Brussels, BelgiumPresented at the 19th European Congress of Pathology (Ljubljana, Slovenia, September 6-11, 2003). A rapidly progressive interstitial fibrosing nephropathy frequently associated with urothelial cancer has been reported in a series of young Belgian women given slimming pills containing Chinese herbs 1-5. We initially proposed to name it Chinese herbs nephropathy 2. The more recent demonstration that aristolochic acid contained in the herbs was the causal agent led us to rename it aristolochic acid nephropathy 6-7. Since the description of the first cases in the early nineties, identical cases have been increasingly reported, outside the Belgian epidemic, after the consumption of herbal remedies containing AA 8. In a minority of cases, the ingested herbs were not reputed to contain AA. These latter cases are designated as Phytotherapy Associated Interstitial Nephropathy (PAIN) until identification of AA or of a possible other phytotoxin.
The renal disease runs a rapidly progressive course even if the phytotoxin is interrupted 9. Half of the patients have initially normal blood pressure. Anaemia is severe in the early stages. Except for mild aseptic leukocyturia, urinary sediment is usually normal. Tubular proteinuria 10 is usually mild and normoglycaemic glycosuria is often found. Renal imaging reveals a symmetric size reduction of both kidneys with smooth outlines. Of note, Fanconi syndrome has been reported in a few patients with AAN outside the Belgian epidemic 8. Heart murmurs due to aortic valve abnormalities have been initially reported in several patients with AAN. They are now attributed to the fenfluramine content of the incriminated slimming pills and not to the toxicity of AA. Urothelial malignancy develops in about half of the patients with end stage renal failure, up to 2-6 years after cessation of toxic exposure 4-5. Pathology
End-stage kidneys of AAN patients are severely and symmetrically shrunken, present smooth outlines and weigh only about 10 g each 2. The peripheral and interpyramidal cortex (columns of Bertin) are diffusely thinned, pale and granular, measuring only few mm in thickness. The arteries and the dark medulla are relatively well preserved. Pelvis and ureters have a normal gross appearance. Severe periureteral fibrosis has been described in one patient only.
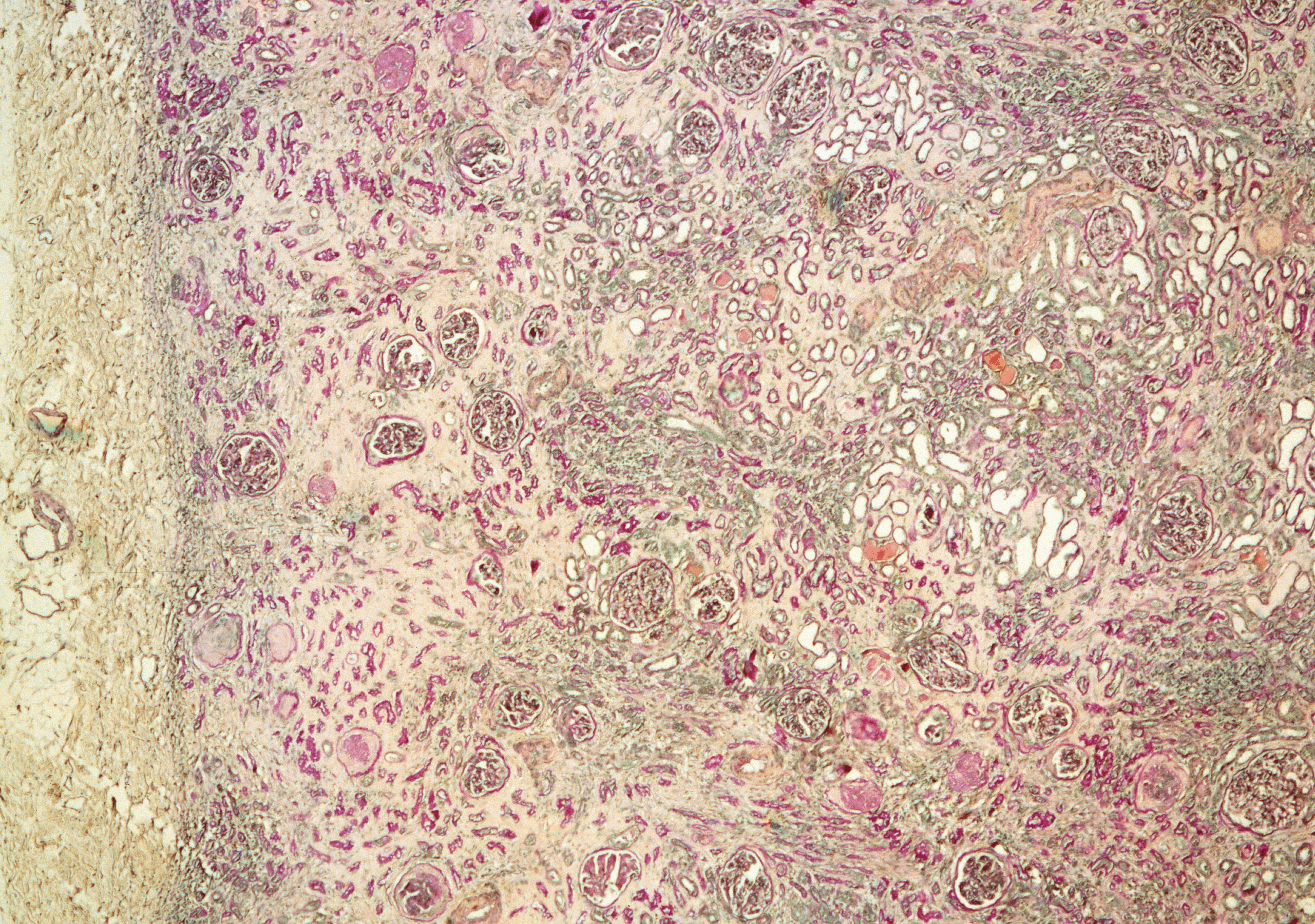
The most striking histological feature of AAN is the presence of extensive, dense, pauci- or a-cellular interstitial fibrosis decreasing in intensity from the upper to the inner cortex 2-3 (fig 1). Medullary rays and to some extent the outer stripe of the outer medulla are similarly involved whereas the inner stripe of the outer medulla and the inner medulla are usually much less injured. The severity of the associated tubular atrophy and to some extent of the global glomerular obsolescence of the collaptic type follow the same topographic distribution as the interstitial fibrosis. Interlobular arteries show prominent intimal fibrosis whereas larger arteries display usually mucoid fibrous hyperplasia. Multifocal atypia are constantly found along the epithelial lining of collecting ducts and along the pelvi-ureteric urothelium 2, 4-5. In susceptible patients, urothelial carcinoma develops as multiple foci of carcinoma in situ of the transitional cell type most often bilateral and located in the upper urinary tract (pelvis and ureters). Outside the Belgian epidemic, upper urinary tract malignancy has been reported in the 2 only available nephroureterectomy specimens removed from 2 patients 8.
Immunofluorescent staining shows non specific, mild, granular deposition of IgM and C3 in the glomerular mesangium, along some glomerular capillaries and in small arterial walls. C3 is also found along the basement membrane of cortical atrophic tubules and along peritubular capillaries 2.
Electron microscopy Non specific changes including scanty, segmental, sub-endothelial immune deposits or translucent zones, segmental glomerular basement membrane thickening, wrinkling or duplication, thickened tubular basement membranes and Bowman's capsules, and reduced tubular epithelial cells with loss of microvilli have been reported 3.
The hypothesis that AA had inadvertently been included in the slimming pills perhaps as a result of confusion between fangji (S. tetrandra) and fangchi (Aristolochia) 1 was confirmed by the identification of AA and the absence of tetrandrine, the alkaloid extracted from S. tetrandra, in 10/12 imported batches of so-called S. tetrandra herbs used to prepare the pills 11.
AA is the nephrotoxic and carcinogenic active principle extracted from the Aristolochia species 12. It is a mixture of structurally related nitrophenanthrene carboxylic acids, AAI and AAII being the major components. Both acids have been identified by high performance liquid chromatography (HPLC) in the slimming pills 13. They bind covalently to the exocyclic amino group of DNA purine nucleotides leading to the formation of AA-DNA adducts: the 7-(deoxyadenosin-N6-yl)- aristolactam I (dA-AAI), the 7-(deoxyadenosin-N6-yl)- aristolactam II (dA-AAII), the 7-(deoxyguanosin-N2-yl)- aristolactam I (dG-AAI) and the 7-(deoxyguanosin-N2-yl)- aristolactam II (dG-AAII). Using the 32P-postlabelling method and cochromatographic analyses with authentic markers , most of those AA-DNA adducts (dA-AAI, dA-AAII and dG-AAI) were identified in the kidney and ureteric tissue of CHN patients 5, 14. These findings confirm exposure of the patients to AA. Moreover, AA given alone to rodents induces clinical, morphological and carcinogenic features typical of AAN in humans, conclusively demonstrating the causal role of this alkaloid in the development of the disease 6.
High doses of AA induce acute tubular necrosis in several species 8. Chronic administration in NZW rabbits induces extensive hypocellular interstitial fibrosis with tubular atrophy mainly in the medullary rays, outer stripe of outer medulla and outer cortex, which are reminiscent of the pathologic changes characterising AAN in humans 6. The pathogenesis of AA-induced interstitial fibrosis is still a matter of debate. A primary proximal tubule injury is suggested by the development of low molecular proteinuria. Exposure of OK cells, an established model of proximal tubule cells, is instantly followed by the formation of AA-DNA adducts, a decreased cellular expression of megalin and by a permanent inhibition of endocytosis 15. It may be hypothesised that chronic proximal tubular epithelial cell damage leads to interstitial inflammation and fibrosis. It is of interest to note that the predominance of fibrosis in the medullary rays and in the superficial cortex fits well with the hypothesis of a primary toxic insult of the S3 segment of the proximal tubules of mainly the superficial nephrons. Alternatively, the likelihood of a primary vascular insult is hampered by the absence of vascular lesions in patients with AAN at early stages 3 as well as in the kidneys of rabbits fed AA 6. Moreover, benign nephrosclerosis is characterised grossly by finely or coarsely granular kidney outlines. Microscopically, interstitial fibrosis and tubular atrophy induced by chronic renal ischaemia is multifocal and shows no predilection to the subcapsular area or medullary rays. It is associated with severe intimal fibrosis of large and interlobular arteries, and with arteriolar hyalinosis. Finally, the possibility that the renal fibrosis is due to a DNA mutation awaits further elucidation.
The formation of AA-DNA adducts provides a pathophysiological clue as to the mutagenic and carcinogenic effects of AA 5, 14. The detection of specific DNA adducts up to 89 months after toxic exposure makes them highly suitable for monitoring exposure to AA even years later. They suggest non reparable genomic lesions. This is in line with the reported long-term persistence of AA-DNA adducts in the kidneys of rats given AA 14. Ha-ras proto-oncogenes are activated with high frequency by an A -> T transversion mutation in codon 61 from CAA to CTA in the DNA of AAI-induced forestomach carcinomas in rats 16. The overexpression of p53 by atypical and malignant urothelial cells in AAN patients suggests that tumour suppressor genes may also be mutated 4.
The diagnosis rests on the history of the ingestion of phytotherapeutic agents proven to contain AA by chromatographic analysis, on the typical findings of mainly subcapsular and hypocellular interstitial fibrosis, and whenever possible on the characterisation of AA-DNA adducts in DNA extracted from urinary tract tissue. The clinical, biological and pathological features of AAN are reminiscent of two other fibrosing interstitial nephropathies associated with the frequent development of urinary tract malignancies 2, 8: Analgesic (AN) and Balkan nephropathy (BN). Papillary necrosis, which is absent in AAN, is the hallmark of AN and is likely to be the cause of the overlying areas of cortical interstitial fibrosis and tubular atrophy showing no predominance in the outer cortex or in medullary rays. It leads to asymmetrically shrunken kidneys with irregular outlines and papillary calcifications. In contrast, AAN is very reminiscent of BN which is possibly due to AA 17. However, the course of progression towards end-stage renal failure lasts longer in BN (decades) than in AAN (few months). This different rate of progression may be due to differences in the amount of AA ingested, to interindividual differences in the susceptibility to toxic substances or to the possible potentiation of the toxicity of AA by its admixture with other compounds contained in the slimming pills.
The benefits of corticosteroid therapy to slow the progression of renal failure remains debated 18-21. Renal replacement therapy followed by renal transplantation have been performed in more than half the patients of the Belgian epidemic 9. No cases of recurrence are hitherto reported. The absence of fibrotic changes in the peritoneum of both AAN patients and AA-treated rabbits allows the use of peritoneal dialysis in these patients 22. Bilateral nephro-ureterectomy performed at the time of renal transplantation or shortly thereafter with subsequent regular urinary cytological examinations is recommended 4-5.
The Belgian tragedy has unravelled an hitherto unsuspected severe toxicity of herbal drugs containing AA which should be banned. It has further pointed out to the urgent need to submit the so-called "natural" harmless drugs of herbal medicine to a critical evaluation of benefits and side effects prior to their release for medical use just as is mandatory for drugs released in the Western world. 23-25.
1 Vanherweghem JL, Depierreux M, Tielemans C et al. Rapidly progressive interstitial renal fibrosis in young women: association with slimming regimen including Chinese herbs. Lancet 1993; 341: 387-391
2 Cosyns JP, Jadoul M, Squifflet JP et al. Chinese herbs nephropathy: A clue to Balkan endemic nephropathy? Kidney Int 1994; 45: 1680-1688
3 Depierreux M, Van Damme B, Vanden Houte K et al. Pathologic aspects of a newly described nephropathy related to the prolonged use of Chinese herbs. Am J Kidney Dis 1994; 24: 172-180
4 Cosyns JP, Jadoul M, Squifflet JP et al. Urothelial lesions in Chinese-herb nephropathy. Am J Kidney Dis 1999; 33: 1011-1017
5 Nortier JL, Muniz Martinez MC, Schmeiser HH et al. Urothelial carcinoma associated with the use of a Chinese herb (Aristolochia fangchi). N Engl J Med 2000; 342: 1686-1692
6 Cosyns JP, Dehoux JP, Guiot Y et al. Chronic aristolochic acid toxicity in rabbits: A model of Chinese herbs nephropathy ? Kidney Int 2001; 59: 2164-2173
7 Cosyns JP. When is "aristolochic acid nephropathy" more accurate than "Chinese herbs nephropathy"? Kidney Int 2002, 61: 1178-1181
8 Cosyns JP. Aristolochic acid and 'Chinese herbs nephropathy'. A review of the evidence to date. Drug Safety 2003, 26: 33-48.
9 Reginster F, Jadoul M, van Ypersele de Strihou C. Chinese herbs nephropathy presentation, natural history, and fate after transplantation. Nephrol Dial Transplant 1997; 12: 81-86
10 Kabanda A, Jadoul M, Lauwerys R et al. Low molecular weight proteinuria in Chinese herbs nephropathy. Kidney Int 1995; 48: 1571-1576
11 Van Haelen M, Vanhaelen-Fastre R, But P, Vanherweghem JL. Identification of aristolochic acid in Chinese herbs. [letter] Lancet 1994; 343: 174
12 De Smet PAGM. Aristolochia species. In: De Smet PAGM, Keller K, Hänsel R, Chandler RF, editors. Adverse effects of herbal drugs. Berlin: Springer-Verlag, 1992; pp. 79-89
13 Cosyns JP, Goebbels RM, Liberton V et al. Chinese herbs nephropathy-associated slimming regimen induces tumours in the forestomach but no interstitial nephropathy in rats. Arch Toxicol 1998; 72: 738-743
14 Bieler CA, Stiborova M, Wiessler M et al. 32P-post-labelling analysis of DNA adducts formed by aristolochic acid in tissues from patients with Chinese herbs nephropathy. Carcinogenesis 1997; 18: 1063-1067
15 Lebeau C, Arlt VM, Schmeiser HH et al. Aristolochic acid impedes endocytosis and induces DNA adducts in proximal tubule cells. Kidney Int 2001; 60: 1332-1342
16 Schmeiser HH, Janssen JW, Lyons J et al. Aristolochic acid activates ras genes in rat tumors at deoxyadenosine residues. Cancer Res 1990; 50: 5464-5469
17 Ivic M. The problem of etiology of endemic nephropathy. Acta Fac Med Naiss 1970; 1: 29-37
18 Vanherweghem JL, Abramowicz D, Tielemans C et al. Effects of steroids on the progression of renal failure in chronic interstitial renal fibrosis: a pilot study in Chinese herbs nephropathy. Am J Kidney Dis 1996; 27: 209-215
19 Martinez MC, Nortier J, Vereerstraeten P et al. Progression rate of Chinese herbs nephropathy: impact of Aristolochia fangchi ingested dose. Nephrol Dial Transplant 2002; 17: 408-412.
20 van Ypersele de Strihou C, Jadoul M. Progression rate of Chinese herbs nephropathy: impact of Aristolochia fangchi ingested dose. Nephrol Dial Transplant 2002; 17: 1852
21 Muniz Martinez MC, Nortier J, Vanherweghem JL. Progression rate of Chinese herbs nephropathy: impact of Aristolochia fangchi ingested dose. Nephrol Dial transplant 2002; 17: 1852.
22 Gillerot G, Goffin E, Moulin P, Arlt VM, Phillips DH, Cosyns JP, Devuyst O. Chinese herbs nephropathy and the peritoneum: Functional, structural, and molecular studies. Kidney Int, in press.
23 De Broe ME. On a nephrotoxic and carcinogenic slimming regimen. Am J Kidney Dis 1999; 33: 1171-1173
24 van Ypersele de Strihou C, Vanherweghem JL. The tragic paradigm of Chinese herbs nephropathy. Nephrol Dial Transplant 1995; 10: 157-160
25 Kessler DA. Cancer and herbs. N Engl J Med 2000; 342: 1742-1743
|